

















 38 / 127
38 / 127

36
A interface vítreo-retiniana
AVM, TVM e BM
25 Perguntas e respostas
REFERÊNCIAS
1.
Duker J, Kaiser P, Binder S, de Smet MD, Gaud-
ric A, Reichel E et al. The International Vitreo-
macular Traction Study Group classification of vit-
reomacular adhesion, traction and macular hole.
Ophthalmology 2013;120:2611-9.
2.
Mirza R, Johnson M, Jampol L. Optical coher-
ence tomography use in evaluation of the vit-
reoretinal interface: a review. Surv Ophthalmol
2007;52:397-421.
3.
De Smet MD, Elkareem A, Zwinderman A,
The Vitreous, the Retinal Interface in Ocu-
lar Health and Disease. Ophthalmologica
2013;230:165-78.
4.
Krebs I, Brannath W, Glittenberg C, Zeiler F,
Sebag J, Binder S. Posterior vitreomacular
adhesion: a potential risk factor for exuda-
tive age-related macular degeneration? Am J
Ophthalmol 2007;144(5):741-6.
5.
Mojana F, Cheng L, Bartsch DU, Silva GA,
Kozak I, Nigam N et al. The role of abnormal
vitreomacular adhesion in age-related macu-
lar degeneration: spectral optical coherence
condições caracterizadas pela isquémia, infla-
mação e edema maculares resulta em desfe-
chos clínicos menos favoráveis
12
. Muitas vezes
é difícil, se não mesmo impossível, determinar
qual a entidade clínica ou fisiopatológica direc-
tamente responsável pela deformação arquitec-
tural da retina nestes casos. Embora a nature-
za desta interacção não esteja completamente
esclarecida, abrem-se novas perspectivas
terapêuticas com intervenções dirigidas à nor-
malização da IVR, podendo ser um contributo
para potenciar os resultados clínicos finais.
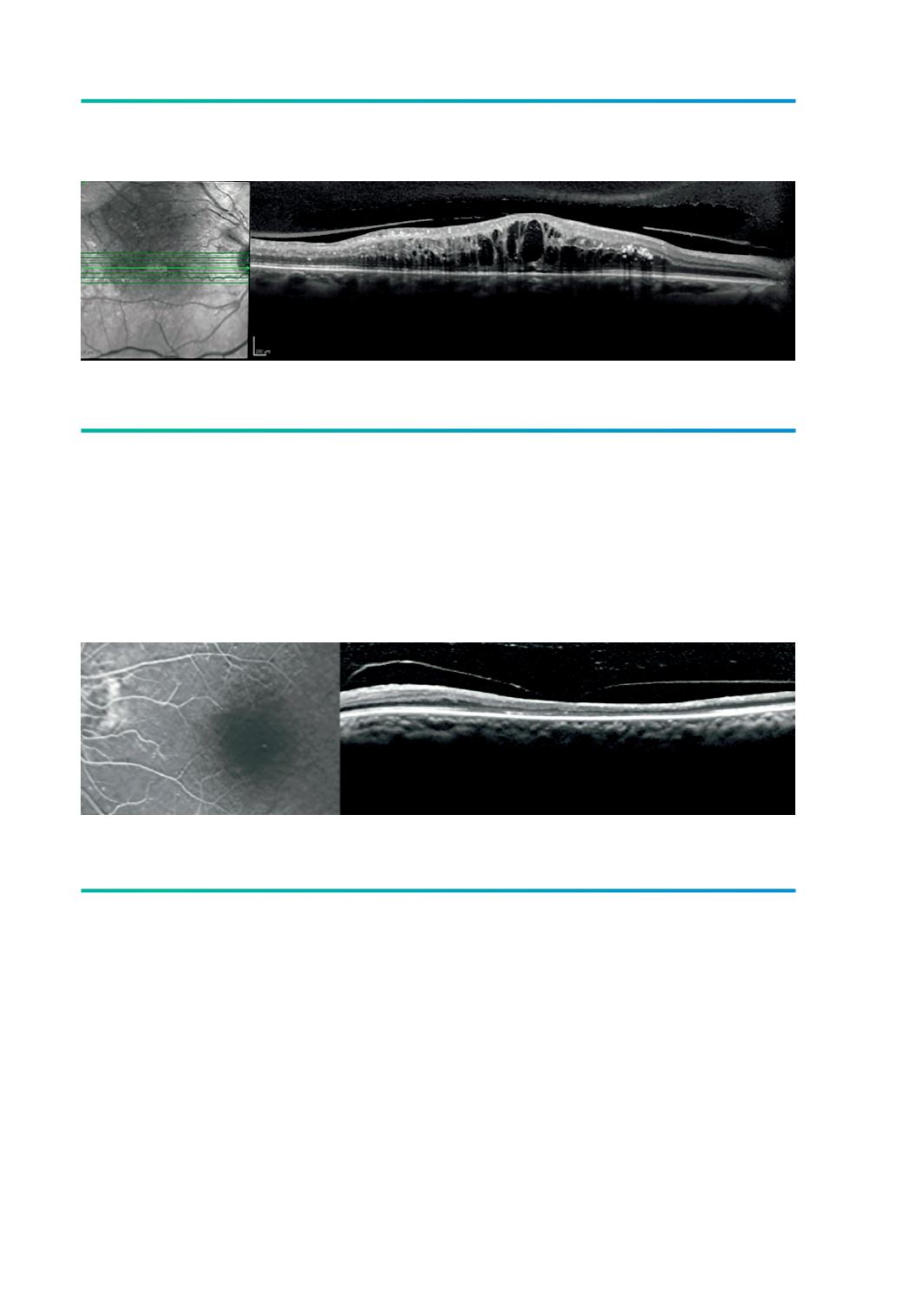
Figura 6.
AVM focal em oclusão de ramo da VCR.
Figura 7.
TVM em oclusão venosa antiga com isquemia e atrofia macular.